Introduction:
1. The Tendency and Danger of Stereotypical Thinking
As humans, we often use rules of thumb, also known as stereotypes, to make sense of our physical and social environment. In many cases, this psychological phenomenon has served us well as a species because it has allowed us to respond quickly because we have had a similar experience in the past. The problem with this psychological tendency is that we also tend to completely ignore differences between people and lump them together in social categorizations. In other words, it reduces people to the all-encompassing 'other', which often leads to in-groups and out-groups. Today, as well as throughout history, such thinking can be tied to social construction of race and its hold on our thinking; the psychological phenomena of stereotype threat,etc.[1]
One of the most famous evaluation of stereotypes was from the study performed by Katz and Braly in 1933. Katz and Braly investigated the stereotypical attitudes of Americans toward social constructions of race and found that ethnic stereotypes are widespread. For this study, they used a questionnaire, with American Students being given a list of nationalities and 84 personality traits. The students where then asked to evaluate each group with 5 or 6 of those traits. The researchers found that White Americans were viewed as industrious, progressive and ambitious; while African Americans were seen as lazy, ignorant, and musical. Participants showed that they were more than willing to evaluate groups that they had little if any contact with.
Though this study was performed 87 years ago, the tendency to evaluate people according to social categories and bigoted stereotypes remains. Instead of treating each person as their own individual, people are reduced to social categories and voting blocks. Through the rest of this report, we will be focusing on an assortment of identities that have become known as the LGTBQ+ community, while attempting to show the intersections of discrimination and marginalization that these individuals face. The key to this approach will be to view each individual as having their own set of lived experiences, identities, and circumstances as a means of deconstructing essentializing discourse and revealing the interwoven nature of their marginalization.[2]
2. What is Intersectionality?
Intersectionality can be understood as the interwoven nature of our individual identity through which our socio-political and economic experiences combine to create a unique mode of discrimination and/or empowerment. Take for example, a Hispanic woman may face extreme poverty in the United States not only because she is Hispanic, or only because she is an undocumented immigrant; or merely because she is a woman, but rather due a combination of these factors and many others that together constitute her experience. The important part of this element of intersectionality is that it assumes as its first principles that there is no single 'Hispanic Trans Female identity'; it attempts to avoid essentializing identity, while providing a better understanding of individuals who have shared experiences that often includes poverty, lack of social services, marginalization, violence, and the construction of concepts to describe such the positive and negative shared features of experience. It takes as it subject the individual subject, with a different assortment of experience and categorizations; while also recognizing that certain political and social structures tend to result in shared experiences.[3]
It attempts to avoid generalizations to provide policy makers, politicians, and the public an understanding as to where such services are needed to prevent the negative consequences associated with a specific categorization. The ability to understand individuals as they see themselves allows researchers to get a clearer conception of their needs in order to prevent harm and improve quality of life for marginalized communities.To be sure, intersectionality not only describes oppression, discrimination, and economic inequality, it can describe anything from a slight privilege to the privilege of the super-rich. We will be discussing intersectionality as a means of illuminating the experiences that together constitute the social, economic and political challenges of marginalized identities. For the purposes of this report, we will begin with a specific group of identities, namely those who identify as part of the LGTBQ+ community in order to identify the interwoven components of their lived experience of political and social structures along with the elements of those experiences and structures of power that lead to a lower quality of life. After going over these various forms of oppression, we will return to intersectionality and attempt to show the interrelated nature of these challenges. As we will show later in this report, many of these structures and experiences of discrimination are caused by others, i.e. being economically disadvantaged can lead to limited access to healthcare, higher rates of incarceration; malnutrition; higher rates of divorce; poor education, etc. The main idea being that these structures and experiences of oppression tend to be causally interrelated, which means that eliminating one can dramatically reduce the impact of another.
3. Access to Mental Health Services & The Prevalence of Mental Health Challenges
3.1 Access to Mental Health Services
The first two challenges facing the LGTBQ+ Community are the prevalence of mental illness, combined with the lack of mental health services and treatment. One of the more damaging components of how we deal with mental illness is the shortage of mental health professionals in general and an absence of providers that identify as LGBTQ+[4]:
“In March, 2017, the National Council of Behavioral Health (NCBH) released a report compiled by a 27-member panel of experts drawn from providers, payers, government agencies and psychiatric associations. The report indicates there is a national shortage of psychiatrists that is about to spiral out of control, with 77% of U.S. counties reporting a severe psychiatrist shortage.[5]”

Figure 1: Top 20 Most Requested Medical Specialty[6]
In fact, the Trevor Project was able to show that a majority of people that identify as LGTBQ+ indicated that they had mental health needs that are untreated or not met by the current provider. From their research, it seems quite evident that this problem arises from negative social stigmatization, discrimination, and oppression that is often directed at that community, causing individuals seeking mental healthcare to fear the possibility of negative experiences with their healthcare professional[7]:

Figure 2: Unmet Healthcare Needs by Gender Identity - Trevor Project

Figure 3: Barriers to Mental Health among LGBTQ Youth - Trevor Project[8]
Not only is there a lack of psychiatrist in general, but that must also mean that there is an even greater shortage of trained mental health experts that identify as LGBTQ+. Why is this significant? Well, in treating individuals for their mental illness, i.e. depression, anxiety, or Bi-polar disorder –among many— it is truly difficult to understand their mental distress, without first experiencing the daily hardships of these individuals:
“Youth frequently described stigma using words like ‘embarrassed,’ ‘ashamed,’ and ‘weakness’ for why they didn’t get mental health care despite wanting it. LGBTQ youth reported concerns about the ability to trust therapists, particularly related to conversion efforts and disclosing information to family members.[9]” (Emphasis added)
It is almost impossible to identify all of the elements in their experience that exacerbate their illness without having a personal experience of such trauma. This is evident from the responses collected by the Trevor Project, which indicates that many individuals that identify as LGTBQ+ avoid mental health treatment due to the inability of the practitioner to understand the hardships that they face on a day-to-day basis. That is, an individual that goes to a counselor or another trained mental health expert may not feel as though they can truly talk about their issues because their interlocutor does not have the experience to understand them on personal level. Some of the individuals interviewed by the Trevor Project indicated that this indeed a challenge for LGTBQ youth[10]:
According to research done by the Trevor Project, One of the LGTBQ youths they interviewed stated “There are no providers in my area that cover both LGBTQ issues and issues for the rest of my mental health,”; with another more stating, “I want a professional who is trained to help people who both have autism and are LGBTQ, but I don’t think that kind of professional exists.[11]”
Apart from the absence of proper care for people suffering with mental illness, individuals that identify with the LGTBQ+ community have higher rates of mental illness than their heterosexual counter parts. This increase in mental health issues has been shown to be directly tied discrimination, victimization, rejection, structural inequality, and social stigmatization, rather than being a consequence of identifying as LGTBQ+.[12] Researchers refer to this phenomenon as ‘minority stress’, which is the idea that social stigmatization, inequality, prejudice, and discrimination often leads to higher rates of mental health issues among individuals that identify as LGTBQ due to the hostile and highly stressful environment that they encounter on a regular basis, causing them to be more prone to mental health issues.[13]
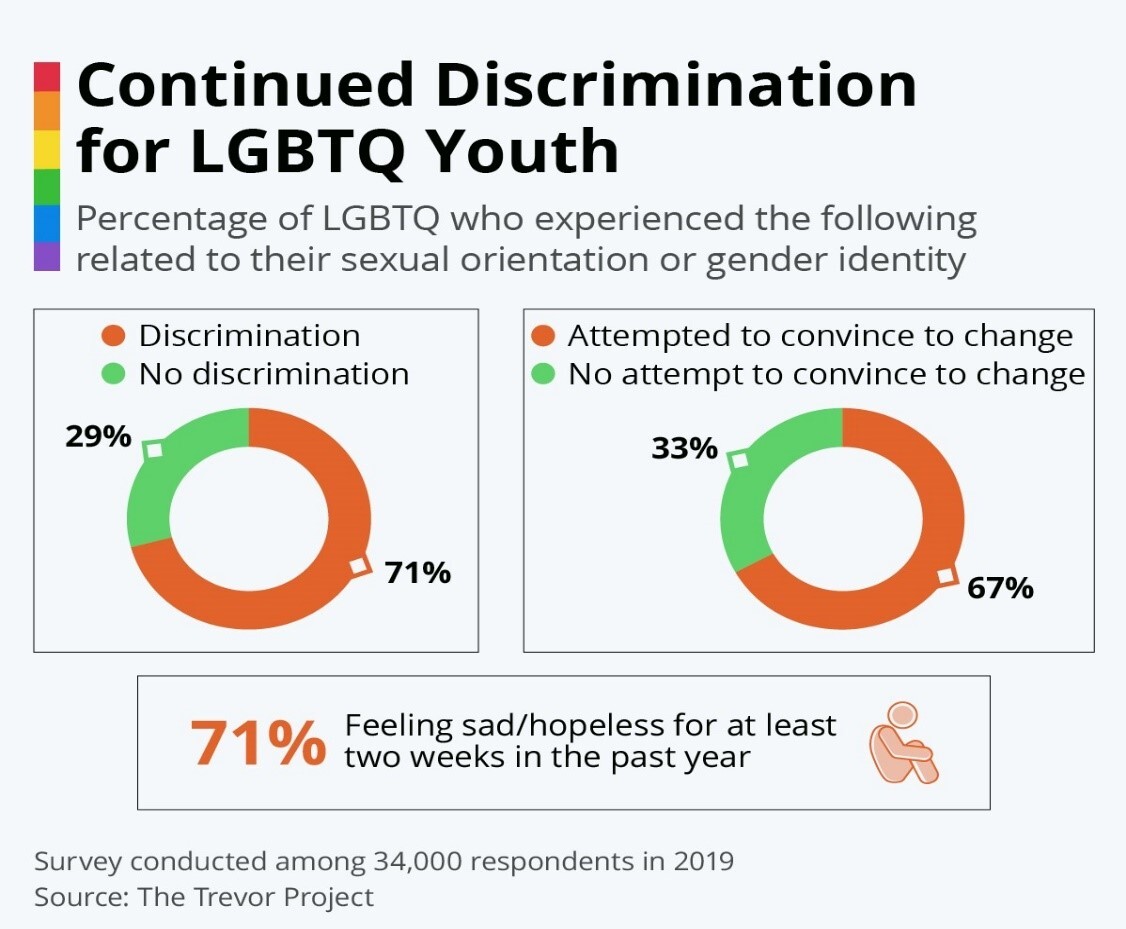
Figure 4: Discrimination and Depression[14]
Now that we have established the underlying cause—namely discrimination, victimization, and oppression—for the uptick in mental health related issues for the individuals that identify as LGTBQ, it is imperative to briefly cover the elements that have given rise to the phenomena of minority stress. Individuals who identify with multiple oppressed identities are at a higher risk of minority stress than those with a single oppressed identity. That is, there is a direct relationship between one’s place on the spectrum of identity and the level of minority stress experienced. Let’s return to our example of the trans black woman; not only will she feel the weight of minority stress through her identity as a trans-women due to discrimination and bigotry, but she will also face discrimination associated with her ethnicity, her economic class position; and even her geographic location can play a role in the level of stress caused by various forms of discrimination and oppression.[15]This is known as minority stress and it identifies discrimination and oppression as the impetus behind higher rates of mental illness that increases with additional forms of discrimination directed toward an aspect of their identity. We will discuss these interwoven forms of oppression in further detail when we return back to the section on intersectionality.
3.2 The Prevalence of Mental Health Disorders
One of the major mental health issues facing individuals that identify as trans or non-binary has been the increasing prevalence of suicidality when compared to their cis-gender counterparts.

Figure 5: Percentage of LGBTQ youth who had consider or attempted suicide within the past 12 months as of 2020, by gender identity
52% of transgender and non-binary population had considered suicide in the past 12 months, contrast this to overall US population that hovers around ~4%.[16] As we discussed before, the more one is exposed to minority stress, the more likely they are to attempt suicide.[17] In other words, the discourse and structures of inequality, discrimination, and oppression lead to higher rates of suicide for the individuals impacted by such structures, with each additional layer of discrimination causing irreparable harm to their mental health. Suicide is not the only area that people in the LGTBQ community face. Research has shown that LGB populations are more likely to suffer higher rates of mental health issues, such as affective disorders and substance use disorders, than their heterosexual counter parts.[18]Kerr et al. found that female bisexual student were 3.1 times more likely to receive a diagnosis of depression, twice as likely to be anxious and approximately 5 times as likely to report a suicide attempt or ideation and self-harm.[19]
Figure 6: Percentage of LGB that have reported mental illness - Source: Mental Health America[20]
In general, LGTBQ youth are six times more likely to experience symptoms of depression than their heterosexual counterparts. LGTBQ youth are also four times as likely to attempt suicide, while LGBTQ youth that come from a family that is highly against their identity being more than 8 times as likely to attempt suicide than LGBTQ youth that come from a home that they report only slightly rejects or accepts their identity.[21]
-- End of Part I
[1] Cardwell, M. (1996). Dictionary of Psychology. Chicago IL: Fitzroy Dearborn.
- See also: Steele, C. M., & Aronson, J. (1995). Stereotype threat and the intellectual test performance of African Americans. Journal of personality and social psychology, 69(5), 797.
[2] Katz, D., & Braly, K. (1933). Racial stereotypes of one hundred college students. Journal of Abnormal and Social Psychology, 28, 280-290.
- See also - Shih, M., Pittinsky, T. L., & Ambady, N. (1999). Stereotype susceptibility: Identity salience and shifts in quantitative performance. Psychological science, 10(1), 80-83
[3] Lynn C. Holley, Natasha S. Mendoza, Melissa M. Del-Colle & Marquita Lynette Bernard (2016) Heterosexism, racism, and mental illness discrimination: Experiences of people with mental health conditions and their families, Journal of Gay & Lesbian Social Services, 28:2, 93-116.
- See Also - Zinn, M. B., & Dill, B. T. (1996). Theorizing difference from multiracial feminism. Feminist Studies,22, 321–331.
[4] “The majority of LGBTQ youth (84%), reported wanting counseling from a mental health care professional in the past year; however, strikingly more than half of those who wanted it (54%) did not receive it.”– See Breaking Barriers to Quality Mental Health Care for LGBTQ Youth – The Trevor Project. 2020, August 18). Retrieved October 11, 2020, from The Trevor Project website: https://www.thetrevorproject.org/2020/08/18/breaking-barriers-to-quality-mental-health-care-for-lgbtq-youth/
[5] 2017 REVIEW OF PHYSICIAN AND ADVANCED PRACTITIONER RECRUITING INCENTIVES. (2017). Retrieved from https://www.merritthawkins.com/uploadedFiles/MerrittHawkins/Pdf/2017_Physician_Incentive_Review_Merritt_Hawkins.pdf
[6] Ibid
[7] “Fears that a provider would not understand the youth’s sexual orientation or gender identity were reported by 33% of transgender and nonbinary youth . . .Transgender and nonbinary youth also expressed more concerns based on negative mental health care experiences in the past (26%) . . . . Within transgender and nonbinary identities, transgender girls/women (33%) and youth who were questioning their gender identity (30%) endorsed fears about being outed based on their LGBTQ identity as a barrier to receiving wanted mental health care more often than nonbinary youth (25%) and transgender boys/men (26%). Additionally, transgender girls/women (27%) were most concerned about a mental health provider only focusing on their LGBTQ identity compared to transgender boys/men (23%), nonbinary youth (21%), and youth questioning their gender (17%).” --Breaking Barriers to Quality Mental Health Care for LGBTQ Youth – The Trevor Project. 2020
[8] Ibid.
[9] Ibid
[10] Other Youth that were interviewed by the Trevor Project also indicated that feelings of weakness when compared to the trials of others can push people away from seeking mental healthcare, “
[11] Breaking Barriers to Quality Mental Health Care for LGBTQ Youth – The Trevor Project. 2020
[12] “The basic issue . . . is not whether some or many homosexuals can be found to be neurotically disturbed. In a society like ours where homosexuals are uniformly treated with disparagement or contempt—to say nothing about outright hostility—it would be surprising indeed if substantial numbers of them did not suffer from an impaired self-image and some degree of unhappiness with their stigmatized status. . . . It is manifestly unwarranted and inaccurate, however, to attribute such neuroticism, when it exists, to intrinsic aspects of homosexuality itself.” - Marmor, J. (1980). Epilogue: Homosexuality and the issue of mental illness. In J. Marmor (Ed.), Homosexual behavior: A modern reappraisal (pp. 391–401). New York: Basic Books
[13] Gilman, S. E., Cochran, S. D., Mays, V. M., Hughes, M., Ostrow, D., & Kessler, R. C. (2001). Risks of psychiatric disorders among individuals reporting same-sex sexual partners in the National Comorbidity Survey. American Journal of Public Health, 91, 933–939.
- See also - Herrell, R., Goldberg, J., True, W. R., Ramakrishnam, V., Lyons, M., Eisen, S., & Tsuang, M. T. (1999). Sexual orientation and suicidality: A co-twin control study in adult men. Archives of General Psychiatry, 56, 867–874
- See also - Sandfort, T. G., de Graaf, R., Bijl, R. V., & Schnabel, P. (2001). Same-sex sexual behavior and psychiatric disorders: Findings from the Netherlands Mental Health Survey and Incidence Study (NEMESIS). Archives of General Psychiatry, 58, 85–91
[14] Topic: Homosexuality. (2017). Retrieved October 11, 2020, from Statista website: https://www.statista.com/topics/1249/homosexuality/
[15] Breaking Barriers to Quality Mental Health Care for LGBTQ Youth – The Trevor Project. 2020
[16] National Public Radio, the Robert Wood Johnson Foundation, & The Harvard T.H. Chan School of Public Health. (2017, November). Discrimination in America: Experiences and views of LGBTQ Americans. Retrieved June 24, 2020 from https://www.rwjf.org/en/library/research/2017/10/discrimination-in-america--experiences-and-views.html
[17] Cyrus, K. (2017). Multiple minorities as multiply marginalized: Applying the minority stress theory to LGBTQ people of color. Journal of Gay & Lesbian Mental Health, 21(3), 194-202.
[18] Gilman, S. E., Cochran, S. D., Mays, V. M., Hughes, M., Ostrow, D., & Kessler, R. C. (2001). Risks of psychiatric disorders among individuals reporting same-sex sexual partners in the National Comorbidity Survey. American Journal of Public Health, 91, 933–939.
- See also - Herrell, R., Goldberg, J., True, W. R., Ramakrishnam, V., Lyons, M., Eisen, S., & Tsuang, M. T. (1999). Sexual orientation and suicidality: A co-twin control study in adult men. Archives of General Psychiatry, 56, 867–874
- See also - Sandfort, T. G., de Graaf, R., Bijl, R. V., & Schnabel, P. (2001). Same-sex sexual behavior and psychiatric disorders: Findings from the Netherlands Mental Health Survey and Incidence Study (NEMESIS). Archives of General Psychiatry, 58, 85–91
[19] Kerr DL, Santurri L, Peters P: A comparison of lesbian, bisexual, and heterosexual college undergraduate women on selected mental health issues. J Am Coll Health. 2013; 61(4): 185–94.
- See also - Liu CH, Stevens C, Wong SHM, et al.: The prevalence and predictors of mental health diagnoses and suicide among U.S. college students: Implications for addressing disparities in service use. Depress Anxiety. 2019; 36(1): 8–17
[20] LGBTQ+ Communities and Mental Health. (2011). Retrieved October 11, 2020, from Mental Health America website: https://www.mhanational.org/issues/lgbtq-communities-and-mental-health
[21] Anxiety & Depression Association of America. (2018). LGBTQ+ communities. https://adaa.org/lgbtq-communities.
- See also - Human Rights Campaign Foundation. (2017, July). Mental health and the LGBTQ community. https://suicidepreventionlifeline.org/wp-content/uploads/2017/07/LGBTQ_MentalHealth_
- See also - National Center for Transgender Equality. (2016). The report of the 2015 U.S. Transgender Survey. https://transequality.org/sites/default/files/docs/usts/USTS-Full-Report-Dec17.pdf